| Indication | Used as an initial treatment for the termination of paroxysmal supraventricular tachycardia (PVST), including that associated with accessory bypass tracts, and is a drug of choice for terminating stable, narrow-complex supraventricular tachycardias (SVT). Also used as an adjunct to thallous chloride TI 201 myocardial perfusion scintigraphy (thallium stress test) in patients who are unable to exercise adequately, as well as an adjunct to vagal maneuvers and clinical assessment to establish a specific diagnosis of undefined, stable, narrow-complex SVT. |
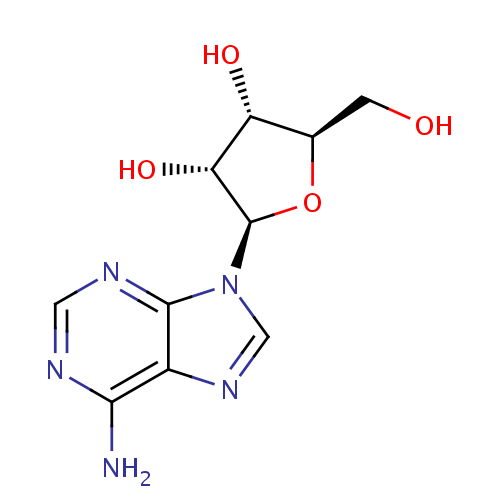
| Pharmacodynamics | Adenosine is an endogenous nucleoside occurring in all cells of the body and is not chemically related to other antiarrhythmic drugs. Adenosine may exert its pharmacologic effects by activation of purine (cell surface A1 and A2 adenosine) receptors, as well as relax vascular smooth muscles through the reduction in calcium uptake by inhibition of slow inward calcium current and activation of adenylate cyclase in smooth muscle cells. Adenosine may reduce vascular tone by modulation of sympathetic neurotransmission. The drug also has negative chronotropic, dromotropic, and inotropic effects on the heart by slowing conduction time throught he AV node and interrupting AV nodal reentry pathways. Adenosine is a potent vasodilator in most vascular beds, but vasoconstriction is produced in renal afferent arterioles and hepatic veins. The drug produces a net mild to moderate reduction in systolic, diastolic, and mean arterial blood pressure and a reflex increase in heart rate. Adenosine is antagonized competitively by methylxanthines such as caffeine and theophylline, and potentiated by blockers of nucleoside transport such as dipyridamole. Adenosine is not blocked by atropine. |
| Mechanism of action | Adenosine slows conduction time through the AV node and can interrupt the reentry pathways through the AV node, resulting in the restoration of normal sinus rhythm in patients with paroxysmal supraventricular tachycardia (PSVT), including PSVT associated with Wolff-Parkinson-White Syndrome. This effect may be mediated through the drug's activation of cell-surface A1 and A2 adenosine receptors. Adenosine also inhibits the slow inward calcium current and activation of adenylate cyclase in smooth muscle cells, thereby causing relaxation of vascular smooth muscle. By increasing blood flow in normal coronary arteries with little or no increase in stenotic arteries (with little to no increase in stenotic arteries), adenosine produces a relative difference in thallous (thallium) chloride TI 201 uptake in myocardium supplied by normal verus stenotic coronary arteries. |
| Absorption | Not Available |
| Volume of distribution | Not Available |
| Protein binding | Not Available |
| Metabolism | Intracellular adenosine is rapidly metabolized either via phosphorylation to adenosine monophosphate by adenosine kinase, or via deamination to inosine by adenosine deaminase in the cytosol. |
| Route of elimination | Not Available |
| Half life | Less than 10 secs |
| Clearance | Not Available |
| Toxicity | Not Available |